Are Crowns All the Same?

Many people have been told that they have a tooth or two that should have crowns to restore a tooth to normal, long-term function.
Most dental practices do crowns, but are crowns all the same no matter where they get done?
All-ceramic fillings, which are inlays, onlays, or overlays are done using the same concept and materials.
These typically leave some standing natural cusps left and this is variable in its long-term outcome.
Mostly the remaining cusps left standing have the strength to survive but sometimes it is better to cover all the cusps even if some remain intact.
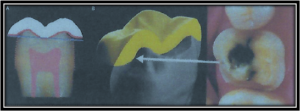
With the technique described below, a Biodome Crown which is really an overlay covering the entire biting surface is the very strongest long-term restoration.
Depending on the strength of these remaining cusps, sometimes they can be left
While different crown materials exist, the other variable to consider is the preparation technique used and that makes the difference.
University dental schools around the world have taught a single preparation technique for the last 80 years or more.
The technique requires the removal of a significant amount of tooth structure from the entire visible part of the tooth to just below the gumline to allow the needed thickness of crown material.
While this may still be appropriate in a front tooth in high visibility, for back teeth, this is a highly destructive practice in removing so much sound tooth structure.
Only a small percentage of dentists have learnt the more conservative technique.
This involves removing only enough tooth structure to allow newer bonding techniques and materials to very strongly rebuild the tooth.
This results in far fewer complications that were caused by over-preparing teeth with the traditional techniques, and a far stronger crown with less likelihood of failure through crown fracture or preventable nerve damage.
These techniques were only developed in the last 15 years or so, and Dr Bob had worked closely under the few international experts who developed the technique.
He went to America for the international release of this method having used it for 2 years prior.
He has also written 2 large dental textbooks in which this technique is published.
It is based on old tried and tested engineering principles practiced in architectural masterpieces like St Peter’s and St Paul’s Cathedrals, and the Roman Pantheon.
The “Dome” is the super-strong engineering design used in these and, also in the current “Biodome“ design in this crown technique.
The massive weight of the dome is a compressive load entirely and the strength is immense.


Why is this concept so important in Dentistry?
All-Ceramic Crowns which consist of various porcelain and zirconia materials, are all tooth coloured.
A property of these materials is the high strength with Compressive forces (loads) applied to these.
The Biodome crown preparation involves the meticulous preservation of as much healthy natural tooth structure as possible to mimic the natural form and function of a sound, healthy tooth.
This preparation technique is crucial to ensuring the longevity of the crown and tooth and maintaining the health of the pulp of the tooth
A traditional, full-coverage ceramic crown, while strong under compressive biting loads, is also quite weak under tensile loads as occurs with the wrap around the sides deeply to below the gum level.
This is evidenced by observing crowns that have broken or cracked under biting load.
Further to that, when sound tooth structure is removed from the sides of the tooth as is done in traditional crown preparations, the risk to the pulp (living nerve inside the tooth) is markedly higher.
The Dentine of the tooth is the hard, sensitive layer of the tooth under the enamel, and this is the very sensitive layer that requires a needle to numb the tooth when it is touched.
The dentine is a solid structure with extremely narrow fine tubes (tubules) that run from where it joins the enamel down to the pulp of the tooth.
Tooth sensitivity is caused by disturbing these extremely fine tubules through capillary action and osmotic gradients. They are the entry point of bacteria and bacterial toxins to the pulp.
Cutting sound dentine places additional risks to the pulp of the tooth.
A Biodome Crown very rarely creates a pulpal problem.
The result is a tooth less likely to have any nerve problems, a much stronger tooth, and a margin between the crown and the tooth which is in an area easily maintained and cleaned compared to below the gum margin in a traditional crown.
The highly aesthetic ceramic materials leave a tooth-crown margin that blends in virtually invisibly.
Dr Bob Gibbins has published 2 large dental textbooks one of which covers this design technique and placed several thousand BIODOME design crowns.
He has a large number of patients who have been advised of the need for a crown or two, but who are staggering these over years to fit in with the private health fund to maximise their rebates.
Many are unaware that the rate of deterioration of a tooth once diagnosed as needing a crown, is often far quicker than is managed by the private health fund coverage, resulting in the need for more complex and more expensive work and the increased likelihood of a sudden emergency.
The watch and wait approach for the health fund to pay their rebates is often a false economy.
Dr Bob won’t be practicing forever, so perhaps an idea to consider catching up with these needed crowns in the nearer future.


